Available Procedures for Nail Care

Nail avulsion is the most common surgical procedure performed on the nail unit. It is the excision of the body of the nail plate from its primary attachments, the nail bed ventrally and the PNF dorsally. Avulsion of the nail plate may be initially performed to allow full exposure of the nail matrix before chemical or surgical matricectomy. Other indications for performing nail avulsion are to treat recalcitrant onychocryptosis; to excise tumors of the nail unit; to allow full examination and exploration of the nail bed, the nail matrix, the PNF and the LNF, and the nail grooves for the presence of pathology; or to use as a preliminary step before performing biopsy on the nail bed and the nail matrix. Avulsion of the nail plate is frequently used as a therapeutic adjunct in long-standing fungal infections of the nail, such as chronic onychomycosis, and in acute bacterial infections. In traumatic nail injuries, avulsion may be used to evaluate the stability of the nail bed or to release a subungual hematoma after failed puncture aspiration.
Paring the nail plate is the process of taking off pieces of the nail in a transverse or longitudinal fashion to fully observe an involved area on the nail bed. In the case of verrucae, nail paring may be performed to determine the extent of disease involvement of the nail plate and the underlying nail bed. The 2 primary methods for performing nail avulsion are distal avulsion and proximal avulsion. A third method, chemical avulsion with urea paste, is a nonsurgical avulsion technique that may be performed. A partial or complete nail avulsion can be performed, depending on location and extent of disease. Surgical nail avulsion is not a definitive cure in cases of nail dystrophy caused by onychocryptosis, nail matrix disease, or extensive nail bed pathology (eg, SCC). Depending on the indication, the nail surgeon must exercise restraint in the decision to perform nail avulsion because cosmetic and functional outcomes should be considered. A distorted curvature of the newly formed nail plate and an elongated, thickened nail due to hypertrophy of the nail plate and the nail matrix are complications associated with multiple or repeated avulsion procedures.
Before avulsion, anesthesia of the digit is achieved through a digital block performed with 1% lidocaine. A Penrose drain secured with a hemostat clamp is used for hemostasis. Any of the following 3 blunted instruments may be used to separate the nail plate from its attachments: the mosquito hemostat, the Freer septum elevator, or the dental spatula. In distal nail avulsion, the instrument is introduced under the distal free edge of the nail plate to separate the nail plate from the underlying nail bed hyponychium on its ventral surface. All attempts at separation are directed proximally toward the matrix, with significant resistance occurring until the matrix is reached. When the matrix is contacted, the surgeon usually experiences less resistance and might feel a laxity because of a weaker attachment. After reaching the matrix, the elevator is reinserted with several longitudinal forward and backward strokes performed side by side until the nail bed is completely freed from the overlying nail plate. To free the nail plate from its association with the PNF and the cuticle, the Freer elevator is inserted under the PNF in the proximal nail groove between the eponychium and the nail plate. Aggressively inserting the instrument into the proximal nail groove causes unnecessary injury and postoperative morbidity, and it should be avoided. Next, the hemostat clamp is used to gently secure and remove the nail plate. If the hemostat blade is used, the serrated, toothed portion of the blade must be oriented to lie directly against the undersurface of the plate and the PNF.
Proximal nail avulsion is attempted when creating a cleavage plane between the nail plate and the nail bed distally is impossible because of the presence of distal nail dystrophy, which prevents access to the distal free edge of the nail plate. This presentation may be seen in distal subungualonychomycosis. First, the Freer elevator is inserted beneath the cuticle in the proximal groove to separate the PNF from the nail plate. Then, it is repositioned to allow its concave surface to match the curved contour of the ventral surface of the nail plate. The instrument is advanced until it finally reaches the distal edge of the nail plate. A hemostat is used to gently remove the nail plate.
The use of urea ointment to debride and avulse dystrophic nails has been applied in the treatment of onychomycosis, onychogryphosis, psoriasis, and candidal and bacterial infections. Nail plates that are significantly dystrophic appear to respond better to avulsion with urea paste. The benefits of performing nonsurgical nail avulsion with urea ointment include pain relief; a low risk of infection, hemorrhage (ie, bloodless procedure), and other morbidity; a quick improvement after avulsion; and the absence of pain during and after treatment.
Nail avulsion with urea is ideal for the treatment of symptomatic dystrophic nails in patients with diabetic neuropathy, vascular disease, or immunosuppression. A disadvantage of urea avulsion is the required length of application and the potential irritation that may result from the acidity of urea. Urea acts by dissolving the bond between the nail bed and the nail plate, and it also softens the nail plate. Urea ointment paste is formulated to include 40% urea, 5% white beeswax or paraffin, 20% anhydrous lanolin, and 35% white petrolatum. Alternatively, Ureacin-40 ointment is an over-the-counter commercial product that is ready made and can be used as a substitute.
Prior to the application of urea, the paronychial area is protected with adhesive tape to prevent chemical irritation of the soft tissues. Urea ointment is liberally applied to the nail plate, and an adhesive felt (eg, moleskin) or a waterproof, stretchable, hypoallergenic tape (eg, Blenderm) is used to create a well around the treated thickened nail to hold the paste. The patient is instructed to keep the nail occluded and to avoid wetting the treated area. After 1 week of occlusion, a blunt dissection is performed to facilitate removal of the dystrophic nail by using a nail elevator and a nail clipper, while leaving the underlying normal nail intact. The avulsion procedure is painless, thus negating the need for anesthesia. The avulsed area is treated with a topical antifungal agent. When necessary, this treatment is complemented with oral antifungals until the new nail is well formed.
Gross thickening of the nail without significant nail dystrophy may be the etiology of a poor response to urea treatment. In this case, gentle abrasion of the nail surface may be tried to help improve penetration of the chemical agent. Contact of the urea-treated nail with water and poor occlusion by the dressing are other causes of treatment failure. When minimally dystrophic nails are being avulsed, a combination of 20% urea and 10% salicylic acid ointment under a 2-week occlusion may be tried. Onychogryphosis commonly leads to nonreversible nail dystrophy. Urea avulsion is indicated in the treatment of this condition to provide pain relief, and it may be performed twice a year for this purpose.
Matricectomy
The nail matrix is the germinative epithelium that forms the nail plate by means of the continuous differentiation of its basal cells. Matricectomy is the process of surgically, chemically, or electrically ablating or destroying the nail matrix. Complete excision of the viable nail matrix results in loss of the nail plate. Therefore, a new nail plate cannot be regenerated.
Multiple indications for performing matricectomy exist, the most common being a diagnosis of recalcitrant recurrent onychocryptosis or ingrown nails. In this and other debilitating nail conditions, matricectomy should only be considered after all conventional therapies, including temporary partial or complete nail avulsion, have been unsuccessful and the condition remains refractory to treatment. Other indications for performing matricectomy include chronic nail dystrophies, such as onychauxis, onychogryphosis, onycholysis, psoriatic nail, symptomatic onychomycosis that is unresponsive to aggressive antifungal therapy, and painful nail conditions, including pincer nail deformity. For most of these conditions, matricectomy is the definitive cure.
When a decision is made to perform matricectomy, a complete or partial procedure can be completed. Most commonly, a partial matricectomy (the removal of the diseased portion of the nail matrix with an attempt to preserve the central portion of the nail plate) is preferred because preservation of the normal structure and function of the nail plate is possible.
Total matricectomy permanently destroys the ability of the nail complex to produce a nail plate. Complete matricectomy is reserved for cases of chronic or severe nail dystrophy, especially when the condition has become refractory to multiple attempted treatments. Some examples of chronic nail dystrophies that may require total matricectomy include, but are not limited to, onychauxis, onychogryphosis, onychomycosis, psoriasis, and pincer nail deformity. Partial matricectomies are especially useful in the management of persistent onycholysis and onychocryptosis. Some surgeons prefer bilateral partial matricectomy, even when the contralateral side may not yet be affected by onychocryptosis. This procedure allows the nail plate to maintain its function and aesthetics. Onycholysis is the separation of the nail plate from the nail bed distally and laterally. When onycholysis extends to the matrix, the detachment is considered complete. In onycholysis, the nail color may become grayish white from air trapped under the nail.
In onycholysis associated with psoriasis, a yellow border may be present between the healthy pink nail and the separated white portion of the nail plate. Onychomycosis and trauma are the 2 major causes of onycholysis of the toenail. Other causes of onycholysis include local trauma; fungal, viral (wart), or bacterial infection; inflammatory disease (eg, lichen planus); alopecia areata; psoralen plus ultraviolet A (PUVA); certain antibiotics (eg, tetracycline); some chemotherapeutic agents (ie, 5-fluorouracil, doxorubicin, bleomycin); and congenital disease as in congenital paronychial infection and partial hereditary onycholysis.
Onycholysis is usually painless, but the patient might complain of mild pain during the early inflammatory period. Before matricectomy, the preoperative evaluation should include a medical history and physical examination to exclude patients with documented small and large vessel occlusive disease (eg, atherosclerosis, diabetes mellitus, collagen vascular disease) in whom, because of delayed healing, this type of surgery is considered to be relatively contraindicated. Patients presenting with claudication, absent distal pulses on palpation and Doppler examination, poor capillary refill, poor wound healing, or low oxygen saturation should be excluded. Matricectomy should be deferred until all acute infection of the digit and paronychial tissues has resolved.
Matricectomy can be performed by using surgical, chemical, or electrical modalities. Ablative matricectomy involves the use of chemocautery, electrocautery, or laser to destroy the nail matrix. Excisional matricectomy uses cold steel surgery, cutting electrosurgery, or cutting laser to remove the matrix. Conservative treatment to correct an ingrown nail includes removing the nail spicule (the inciting cause), trimming the nail transversely to promote forward growth, and daily packing of nonabsorbent cotton under the involved area of the nail plate to allow the nail to grow out straight. A partial or complete nail avulsion may be curative, but, in some cases, it only serves as a temporary measure.
Surgical intervention is indicated when conservative measures fail. In preparation for surgical extirpation of the matrix, all nail spicules are removed by curettage. Hypertrophied granulation tissue can be reduced with an intralesional corticosteroid injection of triamcinolone acetonide, high-potency steroid preparations, cauterization, or excision. Removal of granulation tissue frees the previously fixed nail plate, allowing the plate to be elevated out of the LNF groove.
Surgical resection of the LNF, lateral nail plate, hyponychium, nail bed, and nail matrix is scheduled at 4 weeks after curettage and excision of the granulation tissue. Essentially, the entire lateral nail-forming unit is removed.
Two important issues must be considered before performing matricectomy:
1. All excisions must extend to the periosteum with caution to avoid the insertion of the extensor tendon on the distal phalanx.
2. No remnant of the lateral matrix horn must be left behind to prevent recurrence of nail spicules.
In the surgical management of onychocryptosis, several procedures and techniques are available to the nail surgeon, with each technique having benefits and disadvantages. When performing a partial matricectomy, the digit is first prepared in a sterile environment (iodine or chlorhexidine scrub may be used), and anesthetic is administered through a digital block. A 3/8-inch Penrose drain is used as a tourniquet to provide hemostasis. Some surgeons may prefer an exsanguinating tourniquet to maintain a bloodless field The area to be excised is outlined with a surgical pen, and a partial nail avulsion is performed. A nail splitter is used to cut the nail plate longitudinally, consisting of approximately one fourth of the distance from the lateral nail wall. After cutting the nail plate, a nail elevator or a straight hemostat is applied to separate the nail from its attachments at the PNF, the nail bed, and the matrix. The laterally avulsed nail is grasped and rotated out toward the disease-free nail to prevent embedding of nail spicules into the LNF. The PNF is reflected back to allow full visualization of the matrix.
After avulsion, a scalpel blade is used to make 2 longitudinal incisions, measuring 4 mm in width, beginning at the distal edge of the nail to include the hyponychium and advancing proximally. The nail bed, the nail matrix, and the lateral aspect of the PNF are excised. The incision also extends to include the LNF and the lateral matrix horn in the lateral nail groove. The surgical sample is a wedge of tissue containing the nail-producing components of the nail unit. Fine scissors are used to remove the tissue sample. After obtaining the sample, the PNF is repositioned to its original anatomical site. Hemostasis is achieved with electrocoagulation, Monsel solution, or aluminum chloride solution. The wound may be allowed to heal by secondary intention. Alternatively, the wound may be closed by passing sutures through the nail plate and the LNF. When dressing the wound, the lateral nail groove is packed with iodoform or petroleum jelly gauze. A nonadherent dressing (eg, Telfa) is applied, followed by the placement of a bulky dressing or cling that is secured with elastic tape. Elastoplast may be used. At 24-48 hours after the initial dressing is applied, the wound is soaked in warm water, and the dressing is removed and changed. After surgery, the nail plate remains functional and is cosmetically acceptable. As a result of partial excision of the nail matrix, the newly formed nail plate is narrower because of a decreased width.
In total matricectomy, the entire nail plate is avulsed. A scalpel is used to make 2 incisions oriented proximally and laterally; these incisions extend to the PNF and the LNF. The PNF is dorsally reflected to allow full exposure of the nail matrix, including the lateral matrix horn area. During matricectomy, the first incision is made about 1 mm distally to the distal border of the lunula and is carried 4-5 mm proximally under the PNF in the proximal nail groove to include all matrix tissue. The excised matrix is removed with fine scissors. Sutures or Steri-Strips are used to place the PNF into its normal position. Hemostasis is controlled by direct pressure and electrocoagulation. Postoperatively, patients experience significant pain, morbidity, and prolonged healing. A possible complication of cold steel surgery with scalpel excision may be a higher rate of nail regrowth in the area of the lateral matrix horn; this regrowth is caused by inadequate removal of the matrix from this recessed area. Dorsally reflecting the PNF to fully expose the nail matrix helps to reduce the likelihood of this complication. After surgery, the extremity should be elevated to reduce subsequent pain and swelling. Local bupivacaine can be administered immediately after surgery to provide extended pain relief for at least 8-12 hours. Pain control is usually managed with acetaminophen with codeine.
Chemical matricectomy
Chemical cauterization of the nail matrix with the application of phenol is used to partially or permanently destroy the matrix. Phenol matricectomy is the most widely practiced matricectomy procedure. Phenol denatures protein and retains antibacterial and anesthetic properties. If the goal of surgery is to narrow the nail plate to correct the disparity of a nail too wide for its bed, a partial phenolization is performed.
After unilateral, partial bilateral, or total nail avulsion is performed under digital block, a number-1 curette is used for curettement of the hyponychium, the lateral nail groove, the lateral matrix horn, and the proximal matrix. Curettage appears to lower the rate of recurring nail spicules in the lateral nail horn area, resulting in higher cure rates and a better treatment outcome.
An exsanguinating tourniquet is used to maintain a bloodless surgical field for 2 reasons:
1. Blood is known to inactivate phenol.
2. A dry surgical field helps to facilitate contact between the matrix and the chemocauterant.
Before applying phenol, the surrounding soft tissues are covered with petroleum jelly to protect them against chemical damage and resulting chemonecrosis. A supersaturated solution of 88% phenol is used. A total of three 30-second applications of phenol are required in partial matricectomy and five 30-second applications are used in complete matricectomy. A sterile cotton-tipped applicator dipped in the concentrated phenol solution is directed laterally into the recessed area of the lateral matrix horn and dorsally to contact the matrix tissue on the ventral surface of the PNF.
During the procedure, the cotton applicator is used to vigorously massage the matrix with a twisting motion. After phenol application, lavage of the treated area is performed by using 70% isopropyl alcohol to neutralize the concentrated phenol. Sodium chloride solution, boric acid, or 3-5% acetic acid may also be used to neutralize phenol. At this point, the tourniquet is removed. Bleeding is usually minimal and is controlled with aluminum chloride and direct pressure. An antibiotic ointment, petroleum jelly gauze, and number-2 tube gauze are used to dress the wound. Elastoplast or Hypafix tape is placed to secure the dressing. The dressing is removed in 24 hours after a warm-water soak, and the wound is cleansed in diluted hydrogen peroxide solution. This procedure is the standard wound care used in all types of matricectomy procedures. The patient is instructed to perform dressing changes twice daily for 2-3 weeks. Soaking the wound in a warm, diluted Betadine solution may help to accelerate healing.
Phenol matricectomy has a success rate of 95% and higher, and postoperative morbidity is minimal. However, the associated risks of performing this procedure include pain, frequent recurrence, periostitis, unpredictable persistent wound drainage, and extended healing times. The wound usually heals completely within 2-4 weeks by secondary intention. Chemocauterization of the nail matrix is contraindicated in patients with vascular disease. A newer approach to chemocauterization of the nail matrix involves the use of 10% sodium hydroxide. Chemocauterization of the nail matrix with sodium hydroxide is similar to the phenol alcohol method. One difference between the 2 procedures is the required use of a tourniquet for hemostasis in phenol matricectomy.
During the procedure, a cotton-tipped applicator is dipped in a solution of 10% sodium hydroxide and is carefully applied to all areas, including the proximal and lateral nail grooves, where matrix tissue is found. The endpoint of this procedure is the visible white blanching of the capillaries. Once blanching is apparent, the sodium hydroxide is neutralized with 5% acetic acid. The success rate of this procedure reportedly parallels that of the phenol method. However, some nail surgeons prefer 10% sodium hydroxide because of decreased postoperative morbidity with lower recurrence rates, minimal drainage, and faster healing time. A surgeon experienced in sodium hydroxide matricectomy should perform the procedure to avoid excessive chemical-induced tissue destruction with resultant pain and prolonged healing. Chemonecrosis of the surrounding tissues is a potential problem with phenol matricectomy and sodium hydroxide matricectomy.
Ablative matricectomy
In the electrodesiccation and curettage method, the diseased portion of the nail plate is avulsed. A tourniquet is used only during the avulsion procedure. This procedure is followed by vigorous curettage of the exposed matrix and its lateral horn. Electrodesiccation of the area curetted is performed. To ensure complete destruction of all matrix tissue, electric current is applied twice to the treatment site for an estimated 5 seconds. A cooling period of 10-20 seconds should occur between treatments. Excellent hemostasis is provided by means of electrocoagulation. A potential complication of this method is thermal destruction of the nail folds, the surrounding periungual tissues, and the underlying bony phalanx. This complication may be circumvented by using Teflon-coated probes to direct energy primarily to the matrix. Electrosurgical ablation of the nail matrix involves the use of an electrode that is directly applied to the matrix tissue, leading to its destruction. Matrix destruction is carried out independent of incisions and electrodesiccation. A dry surgical field must be maintained, which is accomplished by applying a tourniquet before performing nail avulsion. The electrode has an insulated surface and an exposed surface. The insulated surface protects the adjacent healthy tissues from electrical destruction. Bleeding is usually absent because of adequate electrocoagulation. This method is associated with a rapid healing time, a low recurrence rate, and little postoperative pain. However, scarring may be significantly greater than that seen with the laser technique. Anesthesia must be adequate throughout the procedure.
Ablative matricectomy with carbon dioxide laser vaporization provides selective destruction of the matrix tissue. Carbon dioxide matricectomy is associated with minimal postoperative morbidity, protracted healing time, decreased edema and inflammation, and absence of extensive necrosis of the adjacent dermal tissue. The carbon dioxide laser was first used in the treatment of onychogryphosis.
Before laser treatment, 1% lidocaine is used to perform a digital block. The matrix may be curetted, and the PNF is reflected back with skin hooks to fully expose the matrix. Wet towels are placed around the surgical site to limit injury to the adjacent soft tissues. The laser beam is directed into the deep recessed areas of the lateral matrix horn and the ventral surface of the posterior nail fold, completely obliterating all the matrix tissue and preventing recurrent nail growth. Hemostasis is well controlled.
After laser treatment, a bacitracin pressure dressing is placed over the digit. In 24 hours, the dressing is removed, the surgical site is cleansed, and bacitracin is reapplied. Dressing changes are performed 2-3 times daily over a period of several weeks. The surgical site heals by secondary intention, and healing is rapid with minimal patient discomfort. The advantage of carbon dioxide laser vaporization of the matrix is the use of a defocused laser beam that is limited in its depth of penetration. Thus, laser energy is directed at only matrix tissues. Therefore, carbon dioxide laser vaporization of the matrix is as effective as the other methods in destroying the nail matrix.
Radical matricectomy
Radical matricectomy (the Syme procedure) is the radical en bloc excision of the entire nail complex. This procedure, which is less commonly performed today, is reserved for patients with symptomatic, recurrent onychocryptosis that is refractory to repeated treatments of total nail matricectomy. The plantar flap formed from amputation of the distal half of the terminal phalanx is sutured dorsally over the defect created from the excision of the nail bed and the nail matrix for primary wound closure. Radical matricectomy has a success rate of almost 100%, with low postoperative morbidity, despite the poor cosmetic and functional outcome. Soft tissue resection for ingrown nails is performed in cases of lateral nail wall hypertrophy. This procedure spares the nail matrix and the nail plate, which most likely have a normal shape, and it removes the surrounding paronychial tissues. Soft tissue resection for ingrown nails can be performed in 3 ways: simple nail avulsion, peridigital resection, or elliptical wedge excision.
Simple (partial or complete) nail avulsion may be performed with a 1% lidocaine digital block, especially if significant pain and infection are present. Typically, removing a narrow strip of nail from the embedded side is adequate. Simple avulsion alone has low postoperative morbidity and an estimated cure rate of 30%, relieving pain and resolving infection in this presentation. In cases where granulation tissue has formed, electrodesiccation, cauterization, or excision is used to remove the excess tissue. If the hypertrophied granulation tissues epithelialize, scalpel excision or electrodesiccation with curettage is performed. The patient is instructed to place cotton wool at the previously embedded site to keep the nail plate elevated. Repeated attempts at avulsion are associated with failed treatment outcomes and a greater risk of recurrence. Peridigital resection may be used to treat the soft tissue hypertrophy. When this approach is used, 2 incisions are made: the first incision is a curved line, hugging the lateral surface of the digit, and the second incision is made parallel to the first and is extended to the underlying subcutaneous fat to remove a wedge-shaped sample of tissue. At closure, the nail folds in the nail groove are oriented away from the nail plate, limiting contact between the 2 structures. Elliptical wedge excision of the lateral nail wall and the nail fold is a third option. At closure, Steri-Strips are placed to secure the nail plate to the newly created lateral nail wall. Alternatively, interrupted 4-0 nylon sutures first passed through the skin and then the nail plate may be used to close the defect. The success rate of the last 2 approaches is 50-70%. In presentations where recurrence is extensive or where multiple sites are involved, cold steel excision followed by a single treatment of phenol on the wound is recommended.
Paronychial surgery
The paronychial region is primarily defined by the PNF, the LNF, and the nail walls; the distal cuticle attached to the nail plate; and the ventrally situated eponychium. These components of the nail unit function collectively to prevent infection and inflammation from reaching the proximal nail matrix. A physical or chemical insult most often precedes the introduction of inflammation or infection into the paronychial area. Examples of pathologic conditions that commonly involve the perionychium include acute and chronic paronychial infections, periungual and subungual verrucae, deep fungi, atypical mycobacteria, myxoid cysts, foreign body and pyogenic granulomas after trauma, and tumors (ie, periungual fibroma associated with tuberous sclerosis and acquired digital fibrokeratoma). Emergent antibiotic treatment is paramount in preventing permanent nail dystrophy. Before initiating treatment, culture and sensitivity studies for bacteria are performed. Staphylococcus aureus is the most common organism cultured in acute paronychial infection. Other organisms less commonly identified in acute paronychia are Streptococci pyogenes and gram-negative enteric bacteria. Early empiric antimicrobial therapy with a broad-spectrum penicillinase-resistant antibiotic and a topical antimicrobial agent is recommended. Based on culture results, antibiotic treatment is later streamlined to cover the specific organism identified on culture. Wet compresses with Burrow solution, warm soaks, or alcoholic baths and elevation are also used to help control early infection.
If the acute infection fails to respond to antibiotic treatment within 48 hours, surgical management is indicated. When present, pockets of collected pus can extend around the base of the nail under the PNF and inflame the nail matrix. The pus may dissect the nail away from its weaker underlying proximal attachment. A pressure necrosis can develop within 48 hours with resultant nail dystrophy that may be transient or permanent if surgery is delayed. Before evacuating the pus, a proximal block is administered. A small incision is made parallel to the nail fold and directly over the collection of pus to drain the abscess. Baran and Bureau recommend incising the site of maximum pain rather than the site of maximum soft tissue induration. Formed septa in the abscess base are destroyed by using the tip of a curved hemostat. If infection spreads under the distal nail bed (subungual extension), excision of the entire nail base along with distal avulsion is performed to expose the nail bed. Then, the nail bed is carefully debrided.
Postoperative care involves changing the dressing daily and moistening it with sodium chloride solution or an antiseptic solution. This process is performed daily and is continued until all purulent drainage has resolved. In recalcitrant disease, a crescentic excision of the diseased nail fold along with the proximal nail plate is performed. Healing occurs by secondary intention, restoring the normal anatomical barrier function of this area. Wound toilet includes the application of an antibiotic dressing. The patient should be instructed to avoid contact with water when possible and to protect the hands by wearing rubber gloves. Another surgical approach is to excise the involved tissue and to create an eponychial pouch. The Bunnell technique involves the avulsion of the proximal one third of the nail by cutting across with scissors followed by the placement of nonstick gauze under the PNF. If the infection is confined to one side and has tracked beneath the nail plate, avulsion of the lateral nail adjacent to the infection is performed.
Surgery of myxoid cysts
Myxoid cysts are usually asymptomatic. However, surgical removal of the cysts is indicated when they become too large and cause pressure on the underlying matrix, resulting in longitudinal nail deformities, such as splitting of and ridging on the nail plate. Other indications for surgery include pain, persistent drainage, and development of secondary infection. Conservative treatment may initially be attempted with intralesional corticosteroid injections or by freezing with cryotherapy. When conservative measures prove unsuccessful, elective en bloc excision of the PNF is performed. The goal during surgery is to perform a full-thickness excision of the PNF that includes symmetric small portions of the LNF.
Standard preparation of the digit is performed under sterile conditions. Effective anesthetic is administered, and a wide Penrose drain is applied for tourniquet action. A surgical pen is used to outline the area of planned excision. A Freer elevator is placed in the proximal nail groove to help define the proximal extent of the cyst and to direct movement of the scalpel. The Freer elevator should be positioned to move synchronously with and below the advancing scalpel to avoid cutting deeply into the matrix or cutting the proximal extensor tendon. Hemostasis of the wound may be achieved by means of spot electrodesiccation. Gelfoam or Instat pads are used to control capillary bleeding. A bulky, loose dressing is applied over the wound. The wound is cleansed twice daily with dilute hydrogen peroxide followed by the application of an antibiotic ointment and a replacement of the dressing. If the wound is allowed to heal by secondary intention, the new position of the PNF will be 3-5 mm more proximal to the original position. This outcome is cosmetically appealing with a slender appearance to the digit. If the nail matrix is not permanently damaged, all deformity of the nail plate is expected to disappear in 4-6 months with new nail growth.
Surgery of warts
Treatment of warts is sometimes difficult, and recurrence is a contentious problem in certain patients. Carbon dioxide laser treatment, pulse dye laser ablation, and electrosurgery are reserved for cases of recalcitrant warts. Standard therapies that use cantharidin, cryosurgery, and keratolytics are commonly unsuccessful in eliminating the virus. Despite this finding, cryosurgery by using liquid nitrogen to freeze the wart remains the most commonly practiced treatment approach. Three days before treatment, 10% salicylic acid is applied to the wart with occlusion to help accentuate freezing with liquid nitrogen. Before salicylic acid treatment, subungual warts are first debrided. Liquid nitrogen is applied by a spraying action or by using a cotton-tipped applicator. The estimated freeze-thaw time is 30-45 seconds after which another treatment cycle can begin for a total of 2-3 cycles. During the procedure, the patient may experience pain due to edema produced under the nail bed. If longer freezing times are desired, the patient is made comfortable by administering digital anesthetic. Freezing of the proximal nail bed should be limited to avoid permanent damage to the underlying nail matrix.
In certain patient populations, cryotherapy is associated with high cure rates and minimal complications. The postoperative complications of freezing include pain, blistering, and transient neuropathy; the open wound heals by secondary intention within 2-5 weeks. Less common complications such as depigmentation, nail loss, Beau lines, transient neuropathy, and anesthesia may occur. Pain during the procedure is controlled by providing prophylactic analgesia with 600 mg of aspirin 2 hours before surgery. This regimen is continued 3 times daily for 3 days after surgery.
Electrosurgery
The application of low-voltage current by means of electrodesiccation and enucleation to dehydrate and detach the wart from the dermis has proven efficacy in the treatment of common warts of the nail unit recalcitrant to conservative measures. After administering a local anesthetic, the nail plate is debrided to allow visualization of the wart. Debridement is followed by a 2-step procedure that is designed to soften, destroy, demarcate, and separate the wart from its attachment to the dermis.
In the first step (electrodesiccation), a needle is directly applied to the surface of small warts or intralesionally applied to larger, thicker warts under low-voltage current. The current essentially cooks and vaporizes the contents of the wart. During surgery, bleeding may be profuse when neovascular dermal capillary loops are interrupted; bleeding is often controlled with electrocautery, Monsel solution, or Gelfoam pads. Moderate bleeding can be controlled with electrocautery or by digitally compressing the lateral digital arteries.
In the second step, the charred tissue is removed with a curette, carefully avoiding the dermis and the nail matrix to prevent scarring (enucleation). A smoke evacuator or a suction device is used to remove infectious airborne viral particles. Electrosurgery is associated with an excellent cure rate. However, scarring may be significant. Healing occurs by secondary intention in 3-4 weeks. Potential complications of this procedure include thermal injury to surrounding soft tissues and the adjacent bony phalanx.
Bleomycin treatment
The intralesional injection of bleomycin is highly effective in controlling recalcitrant warts. Before treatment with bleomycin, local digital anesthesia may be performed to control the pain associated with the injection. A diluted concentration of bleomycin (1 µm/mL), mixed with sodium chloride solution, is used. Rare but potential complications include nail dystrophy (if the matrix is contacted), persistent local necrosis, scarring, and local Raynaud phenomenon in patients with previous vascular insufficiency. Bleomycin is contraindicated in women who are of reproductive age and who are capable of becoming pregnant.
Laser treatment
The carbon dioxide laser is beneficial in treating common warts of the nail unit. Patients with multiple infected digits and those who are immunocompromised are more likely to respond to laser treatment than surgical treatment. The surgeon can have precise control of the depth of tissue destruction when using the carbon dioxide laser. Postoperatively, pain, edema, inflammation, and healing times are significantly reduced. Before carbon dioxide laser vaporization of the wart, local anesthesia or a digital block is performed. Carbon dioxide laser vaporization of verrucae uses a defocused beam with minimal thermal scattering. For treatment of recalcitrant warts of the nail unit, a power setting of 2-10 W delivered with a 2-mm spot size is used. The laser beam must be directed into the lateral sulcus to destroy deeply seated wart tissue. Application of the laser beam is continued until all remnants of infected wart tissue are removed. Tissue damage is minimal if exposure duration is appropriately managed.
Superpulsing delivers high-energy pulses with durations of 0.1-100 milliseconds and repetitions of 100 pulses per second. This technique appears to be effective in decreasing the potential for thermal injury to soft tissues and the underlying bone. Overall, thermal damage with laser treatment is much less than that of electrosurgery. Possible thermal injury to the nail matrix may occur because periungual warts usually involve the PNF overlying the proximal matrix. Hypertrophic scarring and permanent onycholysis of the nail plate may be seen in excessive thermal damage to the nail bed.
When managing subungual warts, the nail plate may initially be debrided or directly vaporized without debridement. To fully appreciate the extent of subungual involvement, a partial or complete nail avulsion is usually appropriate. In certain cases, nail avulsion can be avoided. The charred tissue is curetted or excised with scissors. Another approach is the use of electrosurgery to remove most of the wart tissue followed by laser treatment to vaporize the remaining wart tissue. Adjuvant therapies with an associated low morbidity can be used after laser treatment to treat small recurrences. The Nd:YAG laser at a low-power setting of up to 20 W and a spot size of 2 mm has been used in the treatment of periungual and subungual warts as well as plantar warts. The lesion is irradiated until a whitish discoloration appears. The advantages of this laser treatment include minimal bleeding and the absence of smoke plume, thus preventing exposure to infectious viral particles. The benefits of the carbon dioxide laser over the Nd:YAG laser are an accurate depth of tissue ablation, a reduced residual coagulation zone, and a decreased potential for scarring with less postoperative pain and faster healing.
The flashlamp pulsed dye laser has recently been reported as an alternative laser treatment for resistant verrucae, especially of the plantar type. The primary method of destruction is through the application of laser energy to ablate and coagulate the dilated capillaries supplying the wart. The benefits of using this type of laser therapy include eliminating the requirement for an anesthetic and sparing collagen tissue from destruction. Patients also remain ambulatory and functional in the immediate postsurgical period. However, experience and outcome with this approach have been mixed in reviews of the medical literature.
Surgery to repair nail trauma
An accurate physical examination, including radiographic studies to establish the presence of bony fractures and to assist in wound exploration, must be expeditiously performed. The physical examination should focus on determining if paresthesia is present distally and palpating for pulses to establish the sensory and vascular status of the distal finger; evaluating joint stability by checking active and passive range of motion; and observing the involved area for swelling, discoloration, deformity, and shortening. Culturing and staining with Gram stain should be performed on wounds suspected of being contaminated. The standard preparation for hand surgery includes thorough cleansing of the involved extremity to above the elbow to prepare graft harvest sites. The injured digit is prepared in a sterile field and irrigated with sodium chloride solution. Before the extremity is exsanguinated, broad-spectrum antibiotics are administered to allow adequate tissue exposure during surgery when the wound appears to be infected. The sterilized tray of instruments should contain the instruments that are typically used in performing surgery of the nail unit.
Adequate hemostasis is critical in maintaining a bloodless field, thus minimizing the potential for injury to deeper structures. Hemostasis of the digit may be achieved by placing a sterile surgical glove on the hand and cutting a hole in the tip of the finger. The finger of the glove is rolled toward the base of the digit to function as a tourniquet and to increase the effectiveness of the digital block. Alternatively, a Penrose drain tourniquet may be used to achieve hemostasis. Vasoconstriction is avoided to prevent ischemic necrosis of the digit. A proximal forearm tourniquet is used when surgery is performed on the palm or dorsum of the hand. This tourniquet is removed after 25-30 minutes because a longer application results in significant pain. During surgery, electrocauterization is used to control bleeding. A solid knowledge of hand anatomy is crucial in providing the patient with appropriate anesthesia in this setting. Two dorsal digital nerves and 2 palmar digital nerves accompany the digital blood vessels. Anesthetizing the dorsal branch of the digital nerve is associated with less pain, and, for this reason, it is the preferred approach. To anesthetize the dorsal sensory branch of the digital nerve, a digital block is performed by using a 25-gauge needle that contains 2-3 mL of lidocaine. Initially, the needle is introduced into the proximal web space to create a dermal wheal. Then, it is oriented toward the palmar aspect of the digit to complete the digital block. The block is repeated on the contralateral side of the digit.
Alternatively, a 30-gauge needle with 0.5% mepivacaine may be injected into the PNF and the LNF. This method is less preferred. As a general rule, these blocks should not be performed in patients with known vascular insufficiency. Wrist blocks of the median or ulnar nerve, axillary blocks, and intravenous regional blocks are other useful approaches in administering anesthesia. Avoiding injection of a large volume of anesthetic (>3 mL) is important because swelling may cause vascular compromise.
Surgery of subungual hematomas
Management of subungual hematomas largely depends on their size, location, and presentation. Hematomas that occupy 25% or more of the nail bed are evacuated by creating a small puncture hole through the nail plate by using a number-18 needle, a paper clip, a drill, and an acute-tipped scalpel heated over an alcohol lamp or a handheld electrocautery unit. A slow, constant pressure is applied to the center of the nail plate to puncture the plate and to allow drainage of the hematoma. Incomplete evacuation may require a second penetration of the plate. After complete drainage, adherence of the nail plate to the nail bed is ascertained by bogging down the plate with a tight bandage. Trephination of the nail plate provides almost immediate pain relief, and the risk of complications, such as infection and nail dystrophy, are absent with this procedure. Surgical evacuation of the hematoma may help to salvage the nail. If the hematoma is not removed, nail attachments are loosened, and the nail falls off to be replaced by a new healthy nail several weeks after the trauma. Large or total hematomas may indicate a fractured distal phalanx with significant lacerations of the matrix and the nail bed. Prolonged pressure on the matrix leads to permanent nail dystrophy.
Radiography is indicated to exclude fracture because the size of the hematoma and the presence of an underlying fracture are poorly correlated. When evacuating a large hematoma, the nail plate is first avulsed. The nail bed and matrix are carefully explored and examined, and the hematoma is removed. Any laceration of the nail bed is sutured by using 6-0 Dexon sutures or polydioxanone (PDS) 6-0 sutures. The avulsed plate should be cleaned, trimmed, and reattached to the nail bed and the LNFs by using horizontally placed mattress sutures. Stitches are removed in 10 days, when the nail is firmly adherent to the nail bed. Anesthesia is usually not required, but, when indicated, a digital block may be performed.
Repair of simple lacerations
Superficial lacerations that are limited to the nail plate and involve less than 3 mm of the nail bed usually heal independent of surgical repair as the injured nail grows out. Larger lacerations of the nail bed (due to displacement of the nail plate) with phalangeal fracture must be surgically repaired. If the nail matrix is involved, a careful inspection of the matrix followed by surgical repair is required to avoid nail deformity. In this case, the distal nail plate must be avulsed far enough proximally to allow visualization and placement of sutures in the lacerated matrix. The proximal most aspect of the nail plate is left in place to protect the matrix. Any nail bed tissue that is firmly attached to the avulsed plate should be left intact. The injured nail tissue is irrigated and conservatively debrided to avoid removing viable nail tissue. The lacerated nail bed and the matrix are repaired with interrupted 5-0 or 6-0 absorbable sutures.
The avulsed nail is cleaned, trimmed, and reattached to the nail bed. The repaired nail is dressed with sterile petroleum jelly gauze or Xerofoam, followed by a soft, thick dressing that is loosely applied. If the nail plate is damaged beyond recognition and cannot be salvaged, nonadherent gauze is placed on the exposed nail bed. The gauze is replaced at each dressing change. Lacerations of the hyponychium and the LNF are repaired by using 5-0 or 6-0 nylon sutures.
Repair of complex or stellate lacerations
During repair, a complete nail avulsion is performed to fully expose the nail matrix. A Freer elevator is used for separation, and a hemostat is used for avulsion. After avulsion, the wound is carefully debrided. Then, the wound edges are accurately reapposed. To avoid future nail deformity, the nail root and the nail bed are carefully aligned and replaced on the finger by using 5-0 or 6-0 absorbable mattress sutures. Improper management of a complex lacerating injury may result in secondary nail changes, such as nail dystrophy, onycholysis, pterygium, or a malaligned nail plate due to a malpositioned matrix.
Repair of avulsive lacerations
Partial avulsive lacerations of the nail bed with loss of nail plate adherence are surgically treated with split-thickness nail matrix grafts obtained from the same nail bed or from the great toe. Other choices for repairing nail bed avulsions include full-thickness nail bed grafts, split-thickness nail bed grafts, split-thickness skin grafts, or reverse dermal grafts. Avulsive lacerations of the PNF are repaired with a local rotational flap from the dorsal digital skin combined with a small, split-thickness skin graft. In cases of extensive avulsive lacerations, a cross pedicle flap or a cross arm flap is used. Packing the nail fold space with nonadherent gauze prevents formation of adhesions between the PNF and the nail bed.
A thin, split-thickness skin graft may also be used in place of gauze packing. An overlying stent dressing may be placed to prevent a hematoma from developing under the graft. A nail plate that is relatively large can be used as a stent by replacing the plate beneath the PNF after the plate has been cleaned in an antimicrobial solution. The lacerated PNF and groove is repaired with 7-0 chromic gut sutures. The dorsal surface of the PNF is repaired with nylon sutures. The cleaned nail plate or a substitute is replaced and sutured with nonabsorbable mattress sutures.
A full-thickness nail bed graft is positioned over the ventral bony phalanx if the nail pulp is lost and the bone is exposed. A split-thickness skin graft or free nail graft is applied when the avulsed matrix is lost. Healing by secondary intention produces an acceptable outcome. If healing of complex avulsive lacerations is inadequate within 6 weeks, a thin, split-thickness skin graft is used. After nail unit avulsive injuries are repaired, the dressing must allow the nail to heal without further trauma or injury, it must be nonadherent to prevent adhesions from forming between the nail matrix and the PNF, and it must be able to maintain the shape of the nail bed.
Repair of fractures
Stable fractures that are not anatomically displaced do not require manipulation by reduction; however, they should be protected from potential trauma. If a fracture is unstable, it must be immobilized and reduced through closed reduction with external splinting of the injured finger to the adjacent digit. Tuft and shaft fractures of the distal phalanx are usually caused by crush injuries. They commonly present with comminution and mild displacement of the distal phalanx. Treatment is primarily targeted at the injured soft tissues. Tuft fractures frequently present with distal subungual hematoma and multiple bone fragments, with preservation of the nail pulp. This fracture type requires more aggressive treatment to retard the development of pseudoarthrosis and to reduce instability from residual bone fragments left behind. The wound should be well irrigated to completely remove all bone fragments. After inspection, debridement, and irrigation, the wound is sutured and closed.
Shaft fractures are divided into single-transverse, multiple, and open fractures. Management of single-transverse shaft fractures involves fracture reduction with proper alignment to restore the shape and outline of the finger. After avulsion, the nail bed is inspected, and the lacerated edges are reapproximated and sutured to reverse the impinging force. Fluoroscopically guided percutaneous placement of Kirschner wires help to secure the closed reduction. Multiple shaft fractures are managed by fixation and repair of the soft tissue injury after the wound is irrigated. The removal of bony fragments shortens the length of the finger while permitting the fracture ends to reconnect. Plastic surgery may be attempted to restore the length of the finger.
Open fractures that are extensive and involve the DIP joint are treated by amputation or ankylosis (joint fusion) at a 180° angle. After repair of terminal phalanx fractures, the patient is instructed to elevate the extremity for at least 48 hours to help relieve pain and swelling. After 1 month, the patient should return for the removal of external splints and internal fixation wires. Physical therapy may be helpful in accelerating healing. When appropriate, tetanus prophylaxis should be considered; compound fractures and open wounds sustained 6-8 hours before presentation should be treated with oral antibiotics for 1 week.
Lacerations of the nail bed and the nail matrix are repaired as previously outlined. Incomplete debridement of the soft tissue and the nail matrix from between bone fragments results in nonunion and poor healing of the fracture. In the event that pseudoarthrosis develops, it is managed by positioning bone grafts on the ventral surface of the tuft and by using Kirschner wires to transfix the fragments and to restore stability. Kirschner wires are generally useful in transfixing bone fragments to maintain length and alignment when the fracture is not extensively comminuted.
Treatment of splinter hemorrhage
In a young, healthy patient, splinter hemorrhages are explained by a history of minor trauma and require no further investigation. Treatment of splinter hemorrhages should be directed at resolving the underlying cause.
Surgery of nail unit tumors
Surgery of pyogenic granulomas Surgical management of the granuloma is by means of an excision. An electrocauterizing unit or a scalpel is used to perform the excision at the base of the lesion. Biopsy is used to confirm the diagnosis.
Surgery of fibroadenomas
Treatment is determined by the size and the location of the lesion. Treatment involves local excision and the use of a skin graft or reconstruction of the nail bed.
Surgery of glomus tumors
Smaller glomus tumors are excised by creating a 6-mm punched out hole in the nail plate. An incision is made through this hole, enucleating the tumor from its fibrous covering and incising the nail bed tissue. The punched out nail disc is replaced to function as a physiologic dressing. Surgical treatment of larger glomus tumors begins with proximal nail avulsion. The matrix and the nail bed are incised and elevated from the periosteum. Then, the tumor is excised. A nonadhesive gauze pad is placed on the wound to prevent the formation of adhesions between the nail bed and the skin fold. Standard wound care is necessary after surgery.
Surgery of subungualexostoses
Radiographic changes (trabeculated bony growth with an expanded distal area layered by radiolucent cartilage) confirmed on radiographs are diagnostic. Surgical excision of the bony growth is performed under aseptic conditions. A partial nail avulsion is carried out and followed by a longitudinal incision in the nail bed. The tumor is carefully separated from the underlying nail bed, and it is removed with a fine chisel. Alternatively, the nail plate may remain intact, and the bony growth is removed through an L -shaped incision.
Surgery of basal cell carcinoma, squamous cell carcinoma, and melanoma
Surgical management of basal cell carcinoma, SCC, and melanoma in established cases involves excision of the tumor with clear margins if bone metastasis is absent; this is usually accomplished by Mohs micrographic surgery. The surgical site is covered with a skin graft, and the patient is closely monitored for recurrence. If bone metastasis has occurred, the extremity is amputated at the DIP joint or more proximally. Subungual melanoma can be managed by metacarpal or metatarsal ray amputation. Dissection of the regional nodes may be required.
Mohs micrographic surgery has been recommended in the treatment of well-differentiated, potentially aggressive tumors of the nail unit. The Mohs technique of horizontal sectioning allows examination of 100% of peripheral and deep tissue margins of the specimen, resulting in the smallest possible defect and the highest possible cure rates. The Mohs technique has been found to be especially effective in treating Bowen disease (SCC in situ) and SCC involving the periungual and subungual components of the nail unit in the absence of osseous involvement. It has also been indicated for the treatment of recurrent basal cell carcinoma. In presentations of histologically confirmed SCC of the nail unit, destruction of the underlying bone by invasive disease must be excluded on radiographic examination of the affected digit. If bone involvement is established, the patient is scheduled to undergo amputation of the digit at or proximal to the DIP joint. With either a fixed-tissue technique or a fresh-tissue technique, the surgeon can extensively examine the undersurface and peripheral edges of the excised tissue.
The fixed-tissue technique requires in situ fixation of the tissue specimen with zinc chloride paste, a chemical fixative that maintains a bloodless surgical field. The addition of the fixative to neoplastic tissue prevents the tumor from spreading while the lesion is being excised. The fixed-tissue technique is less favored than the fresh-tissue technique because of significant patient discomfort and the excessive time requirement. It takes approximately 12-24 hours to satisfactorily fix the specimen with this method. Moreover, a pronounced local inflammatory reaction to the chemical fixative that may interfere with the evaluation of the tissue specimen at histologic examination may develop in some patients. For pain management, both an oral pain medication and a local anesthetic are usually administered to the patient.
An advantage of using the fixed-tissue technique is its usefulness in handling aggressive SCCs in highly vascularized regions such as the nail bed, an area susceptible to bleeding and from which thin slices of nail tissue are removed. The surgical defect created by the fixed-tissue technique heals by secondary intention. With the fresh-tissue technique, patient discomfort is significantly less and the procedure time is quicker, making this the preferred method. No chemical fixative is needed with the fresh-tissue technique. Here, the surgical defect is repaired with a skin flap or a skin graft, or it is allowed to heal by secondary intention.
The benefits of applying Mohs micrographic surgery in treating nail unit tumors include the following:
1. The Mohs technique is a nail-sparing procedure that provides high cure rate. The treatment outcome is excellent in cases of localized disease.
2. Mohs micrographic surgery is ideal for obtaining tumor-free margins, while maximally preserving the integrity of the surrounding healthy tissues.
3. The Mohs micrographic technique is an alternative to amputation by providing the option of preserving the nail unit and maintaining digital function in cases where the tumor has not yet invaded the underlying deep structures.
4. The Mohs surgical technique is both diagnostic and therapeutic. In general, when nail unit tumors are treated, the performance of Mohs micrographic surgery versus cold steel surgery with wide tumor excision have similar documented cure rates.
Fantasy has entered nail fashions in recent years. Both women and men can be disturbed by nails that split, chip, and break which may affect employability, self-esteem, and interaction with other people. Moreover, any abnormality of the nail can cause impaired function of the hand or foot. Nail cosmetics is gaining popularity among dermatologists as they can improve the condition and appearance of the nails if used wisely. Since the nails are often difficult to treatand takes longer time to respond, nail cosmetics may be an effective support to medical treatment. They may help the patients to cope with their nail dystrophies while waiting for treatment to show its efficacy. It may also be the only choice to hide irreversibly damaged nail. Although, theirpopularity is greatest among women, the market for male manicures is also growing rapidly. The adornment and grooming of nail is an enormous industry, with over US $ 6 billion spent annually at nail salons in the US alone. Although, we do not have this data in India, it is well known that the nailsalons ismushrooming rapidly in Indian metro cities.Nails are painted with exotic colors and designs. Ornaments and even expensive jewels are used to decorate the nails. Nails have thus created a great deal of interest among people as well as among cosmetic industries.However, injudicious use of nail cosmetics and nail grooming tools itself may result in adverse reactions promoting nail disorders and sometimes even deformities.
HISTORY OF NAIL ART
Ancient women used to strive for beauty and were eager to discover various means to capture the imagination of men. It is due to this factor that nail art origins were concentrated mainly in the sphere of men-women relations. History dates back to 5000 years ago when henna was used for the first time for manicure in India.Nail art origins are traced from the term mehendi, used synonymously for henna, derives its name from the Sanskrit word mehandika. In ancient India when a young girl has had her first menstrual cycle, she was considered ready to enter into a marriage and this was when her lips and fingernailswere painted bright redhenna.

Henna on nails - an art originated from India.
Much of the modern revival of henna which is well appreciated worldwide today derives from its popularity in India. Ancient Egyptians were very nail conscious, and Kings and Queens colored their finger and toenails ruby red. Cleopatra used to use henna to tint her nails. Archaeologists have found many solid gold manicure tools in Egyptian tombs.

Cleopatra with henna on her nails
Traced back to 3000 B.C., the first nail polish has been usedin China. During the 17th century, the upper class in Chinese society used fingernails to demonstrate their wealth.Empress Dowager Cixi, the last empress of China, grew her thumb nailsabout an inch long which were far longer than the rest of her fingernails.

Empress Dowager Cixi, the last empress of China seen with her long fingernails.
The whole nail art history may also surprise those who use them: nail polish, for example, can contain the shimmery substance of fish scales called "pearl essence". Nail art origins indicate, that pearl essence is obtained primarily from herring and is one of many by-products of large-scale commercial fish processing.Modern nail art trends include the primary source of the pearlescent shine used in artificial nails, which is a natural, mined mineral.
French Revlon company founded in 1932, started with a single product - a nail enamel and subsequently developed a unique manufacturing process. Soon Revlon was able to offer women a rich-looking, opaque nail enamel in a wide variety of shades.The nail salon industry grew quickly in the late 1970s and flourished during the 80’s and early 90’s.Modern nail art trends are fascinating and innovative.Fancier manicures include painting pictures or designs on the nails or applying small decals or imitation jewels. Pure carmine dye is usually more expensive than gold.
Nail implements
Nail implements are mechanical objects used in the physical manipulation of the nail plate and surrounding structures of the nail unit.

Nail implements: A-Cuticle trimmer; B-Cuticle cutter; C- Cuticle Pushers; D- Nail nipper; E- Emery boards; F- Clipper.
- Emery boards: They have a coarse side, which file down the nail plate and have a fine side, which bevel the surface.

Emery boards
- Nail brushes & buffers:these are used to cleanse and polish the nail.
- Orange wood sticksand cuticle pushers: they are firm implements that loosen the cuticle and push it back from the nail plate.

Orange Wood stick used to push cuticle
Adverse effects
1. Many nail salons uses only soapy solutions to sterilize them between each use and such improper sterilization practice may lead to transmission of bacterial, fungal, or viral infections including the dreaded blood-borne viral infections.When emery boards are used to file nails of digits affected with verruca, it can result in spread of virus particles to other locations on the hand /foot or to other clients.
Measures to prevent infections:
- Clean the instruments in an ultrasonic cleaner, then soak them for atleast 10min in a cold sterilization solution (2 % glutaraldehyde or benzyl alconium chloride)
- The porous implements like emery boards cannot be sterilized because they do not survive soaking or autoclaves. Emery boards, files and orange sticks should be disposable or the users should bring their own implements to the salon.
2. Injury to any of the structures of the nail unit during handling these implements, may result in temporary or sometimes permanent deformities.
Nail grooming/ Manicure
Professional grooming of the nails is known as manicure (grooming of finger nails) and pedicure (grooming of toe nails). The word "manicure" comes from the Latin manus, meaning "hand," and cura meaning "care".
Procedure:
- Hands are first soaked in a warm water and soapy solution to soften the nail plate and cuticles.
- Nails should be trimmed with as slight a curve as possible and with the corners left untouched to avoid ingrown and paronychia. The free edge should be filed in only one direction with a nail file.

Paronychia due to aggressive manicure
- Ideally, nails should be shaped with the sides straight and the tops gently rounded which are stronger than pointed nails. Unfortunately, many people do not prefer to have cuticle and try to cut it.

Cuticle cutting which has to be discouraged
- It is highly recommended not to cut cuticle to avoid Beau`s lines and paronychia. Few individuals try to push their cuticle proximally with an orange stick or a metallic cuticle pusher. The latter is more likely to cause injury to proximal nail fold and hence should be strongly discouraged.
- A base coat, color enamel, and topcoat can then be applied over the nail plate.
Nail grooming techniques
They can be categorized as-
- Nail coats/ Enamels
- Hardeners
- Nail Moisturizers/ conditioners
- Nail Elongators/Prostheses
- Nail Sculpture
- Wrapping
Nail coats/enamels
Nail enamel is the preparation which not only enhances the appearance of the nail by adding color but also acts as protectant in preventing dryness due to contact with water and detergents.
a. Nail enamel: It provides color to the nail and is known by synonyms like nail lacquer, varnish and polish.
b. Base coat- it is usually transparent, fills in irregularities of the nail plate and provides a uniform, neutral color as the starting point for the pigmented nail polish. They contain more resin for better adherence.
c. Topcoat- It is a clear enamel that adds gloss and prevents premature chipping. Top coats contain more nitrocellulose and plasticizer to improve gloss and are abrasion resistant.
Advantages
Nail polish may act as a protectant in preventing contact with water and detergents and may slow down evaporation of water from the nail plate from 1.4 to 0.6mg/cm2 per hour, thus enhances nail moisturization and flexibility. Drying may instead be due to nail polish removers that are usually acetone-based solvents. A layer of enamel can add about 5% to a nail`s strength.
Adverse effects
- Contact dermatitis to nail polish is a well documentedphenomenon(1-3 % of the population may be affected). Toluene sulphonamide formaldehyde resin(TSFR) is the main allergen responsible. Contact dermatitis is less common once the resin is dry.
- Dermatitis may be
1. At the site of application

Contact dermatitis seen at the site of application
2. Ectopic reaction- when the hand transfers a small amount of nail cosmetics to other areas (eyelids, face, and neck)

Contact dermatitis seen at an ectopic area (upper eye lid)
Few manufacturers have introduced hypoallergenic nail varnishes that do not contain resins. Few attempts were made where an alkyl polyester resin wassubstituted for toluene sulfonamide formaldehyde resin. However, these products wear poorly, often resulting in chipping and peeling.
- Distal end of the nail may develop yellow or red discoloration, due to keratin staining, after 7 days of continuous wearing of pigmented nail polish

Yellowish red discoloration and fragility of the nail plate after continuous wearing of nail polish
- However, this discoloration is harmless and it disappears in 14 days after the nail polish has been removed and can be avoided by the application of a basecoat.
- Enamels can be photosensitizers when they contain fluorescents like eosin, erythrosin, fluorescein, or rhodomine B.
- Black, blue, and green nail polishes have been shown to lower pulse oximeter readings of oxygen saturation significantly. This should alert emergency physicians.
- Nail keratin granulations presenting as superficial, fine, and scaly white spots have been documented in women who are used to applying fresh nail polish on top of the old one, without using the nail polish remover.
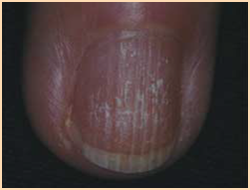
Nail keratin granulations
- This can be avoided by following a 5-7 days nail care schedule including 2 days with the nails free of cosmetic agents.
- Chipped fingernail polish worn longer than 4 days can increase retention of bacteria. Thus, nail enamel can be a source of infection.
Variantsof Manicure
Nail Buffing
It is used as an alternative to nail enamel. Useful in women who already have beautiful nails and to enhance the esthetic appearance. It needs more time and motivation to buff the nails daily.
Composition:
Buffing powder contains- stanning oxide, talc, silica, chalk, or kaolin.
Mode of application:
Buffing powder, paste, or cream is appliedto nail, and a chamois –covered buffer is used to polish the nails till the shine is achieved.

Nail buffing
Adverse effects:
Impatient and rough handling causes injury to the nail matrix and grooving of the nail.
French manicure:
It is a variant that imitates the natural appearance of the nail. The nail plate is painted with a pink or beige color, then a thin strip of white is applied to the tip to simulate the free edge of the nail.

French manicure
Press-on nail polish
Press-on nail polish is a plastic film available in various colors and designs. They can be fixed to the nail plate with its self-adherent property. It is quick and easy to use giving appearance similar to regular nail polish and it does not need a nail polish remover. Unfortunately the wear is poor.
Appliques
Appliques are available in variety of forms like decals, which are pre-glued and hence, can be affixed to the nail plate directly.

A & B- Various appliques available commercially
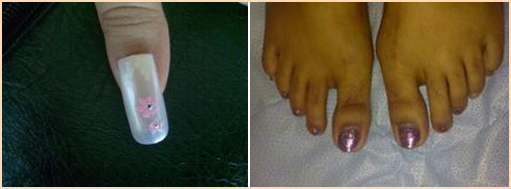
C & D- Finger & toe nails groomed with appliques
They may be painted on with acrylic –based paint and the designs are often elaborate.
Nail Jewelry
Nail jewelry ranges from inexpensive costume accouterments to precious metals and gems. They are attached to nail plate either by glues or mechanically by inserting a post through a hole drilled in the distal nail platejust like how earring on a post is fastened to the pierced earlobe.

Nail jewelry attached through hole drilled in the distal nail plate
Nail printers
It is an innovative recently introduced grooming technique where nails are printed with various attractive fascinating designs. Hand is placed inside the printer and all the nails are printed instantly with desired designs.
Nail enamel removers
Enamel removers are liquid material designed to remove nail enamel safely. Chipping off the old nail enamel with another fingernail should be strongly discouraged as this habit can damage the nail plate.
Composition:
They are made of organic solvents such as acetone,ethyl acetate, butyl acetate, and MEK (methyl ethyl ketone). However, acetone is discouraged today because of its property of dehydration which can result in brittle nails. Conditioning nail enamel removers are available, containing fatty materials such as cetyl alcohol, cetylpalmitate, lanolin, castor oil or other synthetic oils. These substances act as occlusive nail moisturizers retarding water evaporation.
Adverse effects:
Nail dehydration is a known side effect and hence, should be used only weekly. If it comes in contact with skin, it may cause irritation of paronychial folds.
Cuticle removers
Interestingly, the cuticle is one of the stickiest tissues on the entire body which obliterates the space between proximal nail fold and nail plate thus protecting the underlying nail matrix.Under no circumstances should the cuticle be removed or traumatized. Unfortunately, the cuticle is not liked by most manicure artists because it complicates the even application of nail polish. Cuticle removers are substances which dissolve keratin by breaking the disulfide bonds of cysteine and soften the cuticle to allow its easier removal.
Composition:Available inliquid or cream base, they are made of alkaline materials such as sodium hydroxide and potassium hydroxide in a concentration of 2-5%; and humectants like glycerine and propylene glycol to decrease evaporation, irritation and increase viscosity. Milder preparations, which are less effective contain the inorganic salts trisodium phosphate or tetrasodium pyrophosphate andorganic bases such as triethanolamine.
Method of application:
Cuticle removers are applied to the base of the nail for 15-20 minutes. Once the cuticle has become soft, it is pushed back off the nail plate by gently rubbing with orange wood stick.
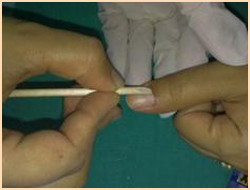
Orange woodstick used to push the cuticle
Professional manicurists may use cuticle knife to lift the cuticle from the nail plate and a V- shaped sharp trimmer or nippers to cut the cuticle

Shaped trimmer used to cut cuticle
Adverse effects:
Most common adverse effect is damage to proximal nail fold. Other risks include fungal or bacterial paronychia, irritant contact dermatitis if left for long period and leukonychiastriata.
Proper councelling of patients about the importance of cuticle and avoiding cuticle removers is strongly recommended. However, if the patient demands for cuticle removers, gentle care in handling cuticle must be emphasized.
Cuticle creams
Cuticle creams unlike cuticle removers are emollients to which quaternary ammonium compounds or urea are sometimes added to promote softening of the cuticle.These are used in between the manicures to maintain a soft, supple cuticle. It is applied on proximal part of nail plate as well as on the proximal and lateral nail fold as frequently as necessary.
Hardeners
Hardeners are essentially a modification of nail polish with different solvent and resin concentrations and with the addition of various other substances.They coat fragile or soft nail plates to provide strength.
Composition:
Originally, the active ingredient of hardeners was 10 % formaldehyde which was discouraged due to its adverse effects. However, US Food and Drug Administration has now permitted low concentration of free formaldehyde(1-2 %). Currently, keratin, calcium fluoride, natural oils, nylon fibers, teflon, and silk have been added to make it formaldehyde free.
Mode of application:
They are applied with brush. Hardeners with 1-2 % formaldehyde should be applied only to the free edge of the nail while the adjacent skin is shielded. Hardeners should be periodically removed with a nail polish remover.
Adverse effects:
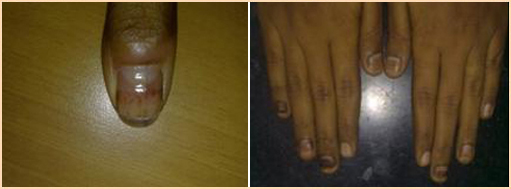
- They may parodoxically cause brittle nails.Products with relatively high (˃ 5%) formaldehyde concentration can cause reversible subungual hemorrhage, bluish discoloration of the nail plate, dryness and scaling of the skin with intense throbbing pain. Some patients may remain symptomatic for many years even after discontinuation of high formaldehyde products.
Adverse effects of nail hardeners

Subungual haemorrage & bluish discoloration of nail plate

Onycholysis due to continuous use of nail hardener
- Dyschromia in the form yellow, red-blue, and brown, has also been associated with use of hardeners.
a& b. Dyscromia due to nail hardener
Nail conditioners or moisturizers are oil-in-water emulsions designed to treat dry and brittle nails.They help counteract the drying effects of repeatedly immersing the hands in water and detergents.
Composition:
They contain the hydrophobic emulsions, proteins, mineral oils, fatty acid esters, triglycerides, and microcrystalline waxes; occlusives, such as lanolin or petrolatum; and humectants, such as glycerin and propylene glycol. α –Hydroxy acids and urea may also be added to increase the water binding capacity of the nail plate. Few products also contain vitamins and collagen. Newer products are made of organic silicon combined with a thiol derivative. These constitute a mercapto-silanol compound that promotes nail growth and strength. It encourages the formation of keratin and the proliferation of peptide bridges between the keratin chains.
Mode of application:
They are applied with a brush or rubbed on. Recently, applicators in the form of highlighter pens are available. They work better if applied under occlusion with a light cotton glove, preferably at bed time for atleast 3 months.
Elongators
Elongators are preformed plastic nails glued with an acrylic - based cement to the natural nail plate to lengthen short nails or cover the entire nail plate.

Nail elongators available in various sizes with glue underneath.
These artificial nails may be prepolished, or decorated with designs. The glue used is ethyl cyanoacrylate.
Mode of application:
- Nails should be prepared by washing and buffing.
- Antiseptic dehydrator is applied with a cotton tip orangewood stick
- Size of the artificial nail should be appropriately selected such that tips do not tend to pop off because of mechanical pressure.
- Adhesive(cyanoacrylate glue) is applied to the prepared nail plate.
- Selected plastic tip is then pressed on nail for 5-10 seconds. Artificial nails should be carefully glued to the affected nails so that glue should not come in contact with adjacent skin.
- Nails can be shaped to achieve desired finish.
They are too occlusive to use for long periods and hence, should be frequently changed.
Adverse effects:
- Ethyl cyanoacrylate is a known sensitizer resulting in allergic contact dermatitis. It should be removed within 48 hours after application.
- Removal of the prosthesis may produce trauma and onycholysis.

Onychoschizia
Sculptured Nails
Sculptured nails are artificial nails formed by molding the resins on the natural deformed nail platewhich results in attractive nails. They are formed to fit and are not preformed. They have become increasingly popular in recent years.
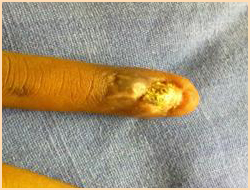
Permanent loss of nail due to trauma induced scar which can be hidden by sculptured nails
Composition:
Nail is sculptured using both polymers and monomers. Polymers include polymethyl methacrylate and benzoyl peroxide available in powdered form whereas monomers include ethyl or isobutyl methacrylate available in liquid form.Benzoyl peroxide acts as an accelerator. The liquid may also contain a stabilizers, such as hydroquinone, resorcinol, eugenol, thymol, or N,N-dimethyl-p-toulidine; plasticizers, such as tricresyl or phthalate phosphate; solvents; and dyes.
Mode of application:
- Initial preparations are same as for elongators.
- Template of nail shape, disposable or metallic shield is positioned on the planned digit taking care to align the template in the natural arch of the nail
- Primer is applied
- A small brush is dipped into liquid monomer and then into the powder polymer and the brush is rotated so that a ball of mixed material is picked up.
- This wet material in the brush is then applied on the tip of the nail over the template.

Sculptured nails- Acrylic material is applied on the template
- This process is repeated over the other parts of the nail and the material is then spread to the cuticle
- The material is then allowed to harden and polymerize.
- Smoothening and shaping the sculptured nail is done using file and polish can then be applied as desired. An acrylic nail can thus be molded producing a long, smooth, and attractive nail.
- As the nail grows out, the gap between the proximal nail fold and the acrylic nail must be filled with more acrylic material to maintain the original appearance. This is necessary once in 2 weeks.
- Patients who wear sculptured nails must use acetone-free nail polish removers to remove polish. Failure to do so may result in removal of the nail sculpture from the natural nail.
Modified sculptured nails
Gel nails: These are the modified sculptured nails which require ultraviolet radiation for polymerization and hardening. The gel is a mixture of ethyl cyanoacrylate and polymethylmethacrylate monomers, and is combined with the same powder polymer used for the regular acrylic nail. Colored gels nails are available for women who do not change polish color very often.
Adverse effects:
- Monomers have potent sensitizing property compared to polymers. Contact dermatitis may occur in distant site.
- Polymers may cause onycholysisand parasthesias of the fingertips.
- Susceptibility to onychomycosis and paronychia(fungal infection) is increased with sculptured nails due to prolonged occlusion.
- Natural nail may grow out thin and brittle after application of the acrylic nail.
- Microorganism colonization is greater on artificial nails than on natural nails. Moreover, artificial nails have also been linked to poor hand washing practices and more tears in gloves. These can result in increased risk of transmitting bacteria to patients by health care workers. Hence, it should be avoided by health care workers.
- Two cases of severe toxic reactions to cyanide were reported as following accidental pediatric ingestion of a product intended for removal of sculptured nails.
Nail wrapping
Nail wrapping is the procedurewhere layers of fibrous substances made of tissue paper, cottonwool, silk, linen, plastic film or fiber glass is applied to the distal edge of the nail plate to either repair and strengthen the free edgeor to elongate the nail plate.

Nail wrapping applied on free edge with fine finishing
Mode of application:
- Initial preparations are same as for elongators.Nails should be long enough to have a distinct free edge in order to be wrapped.
- Small trimmed piece of paperisglued and wrapped over the free edge of the nail so that it should cover only a small portion of the attached nail.
- Nail shaping and desired finishing can be done
- Clear nail polish followed by desired coloredenamel may then be applied
- The procedure must be repeated every 2 weeks after removing the previous wrapping with nail polish remover.
- Paper wrapping is safer than silk and linen wraps as the latter usually cover the entire nail plate, causing occlusion, and thus are not recommended.
Adverse effect:
Nail enamel or acrylic used to glue wrapping may cause allergic contact dermatitis or may cause eye irritation.
COSMETIC THERAPY IN NAIL DISORDERS
Nail cosmetics can be a promising tool in treating many nail disorders. However, abnormal nail itself is often more susceptible to the adverse effects of cosmetics. Nail scrapings, cultures and biopsy samples should be obtained, especially in the case of presumed bacterial or fungal infection, or in case of pigmented bands, which may represent malignant melanoma. If use of cosmetic products is not contraindicated, they can be used effectively to treat or camouflage diseased and misshapen nails.Certainly, priority should be to treat the underlying condition.Few commonly encountered nail disorders and their cosmetic uses are discussed below.
Onychogryphosis:
It is an acquired disorder in which the affected nail becomes thickened, curved and long.

Onychogryphosis seen on 2nd toe nail
OIt may be secondary to trauma.
Cosmetic treatment: Palliative treatment include paring, trimming and thinning the nail with a clipper, file or a mechanical burr. Nail conditioners are useful. This method although somewhat unsatisfactory, is recommended in the elderly because of poor vascularity of their lower extremities. However, complete avulsion either surgically or using CO2 laser is the preferred option in adults.
Koilonychia:
It may be associated with avitaminosis, iron-deficiency anemia, hemochromatosis, or trauma.
Cosmetic treatment:
- Underlying abnormality should be treated.
- Concave depression can be filled with acrylicformsorplastic nails may be applied.
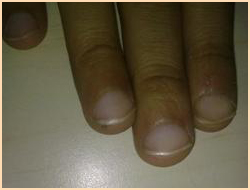
Koilonychia seen on index finger
Nail dyschromia:
Nail dyschromia may be due to use of several systemic and topical agents, cosmetic preparations, or idiopathic. Antibiotics, chemotherapeutic agents, and antimalarials may cause toxicity to the matrix and nailbedresulting in dyschromia. Splinter hemorrhages often associated with psoriasis or trauma may actually herald subacute bacterial endocarditis; and the hyperpigmented lesion of a malignant melanoma may be confused with subungual hematoma.

Nail dyschromia due to chemotherapy
Cosmetic treatment: Nail enamels can be used on a limited basis in such patients as nail plate takes around 6 months to grow out. Men can use slightly tinted enamels or basecoats to avoid embarrassment.
Beau`s lines/Onychomadesis:
Beau`s lines are transverse grooves in the nail plate whereasonychomadesisisshedding of nails.These are associated with serious systemic illness, idiopathic or traumatic. The thickness of the lines is proportional to the duration of the illness. Therapyintended to treat the underlying disease will allow normal nail plate regeneration with eventual growing out of the affected areas.
Cosmetic treatment:
Buffing the nail plate with pumice–containing buffing cream and applying elongators for the duration of the abnormality can benefit these patients.

Beau`s line
Longitudinal grooves:
Longitudinal grooves can be seen on the nail plate which may be caused by aging or trauma,especially to the nail matrix or may be secondary to underlying nail disorders like lichen planus or psoriasis.
Cosmetic treatment:
These grooves may be camouflaged by applying acrylic filler, buffing, and applying enamel. Alternatively, sculptured nails or elongators may be applied. When the groove is trauma induced, it may have its origin in a scar in the matrix, which may be helped by steroid injection or scar excision.
Longitudinal splitting of the distal nail plate:
It occurs due to vigorous filing or trauma, especially in dehydrated nails.
Cosmetic treatment:
Nail conditioners should be applied often. Acrylic fill or nail wrapping is useful in palliative therapy.
Nail pits:
Nail pits are tiny punctate depressions in the nail plate.They have diverse causes like psoriasis, alopecia areata, eczema, secondary syphilis, and trauma.
Cosmetic treatment:
Nail camouflage using several layers of basecoat and nail enamel or by application of nail prostheses can be considered.

Nail pitting
Rough nails:
Rough nails can occur in psoriasis, alopecia areata, ichthyosis, lichen planus, anddue to exposureto chemicals. The hallmarks of this disorder are a rough, brittle nail surface with gray opacities and frequent splits of the distal edge of the nail plate.
Cosmetic Treatment:
Application of conditioners is helpful. Buffing and wrapping offer additional modalities of cosmetic treatment.
Soft nail:
This nails may bend easily or split at the free edge.
Cosmetic Treatment:
Nail fortification with hardener or wrapping are beneficial.Application of plastic nails is another cosmetic option to be considered in such patients.
Hard nail:
Hard and thick nail as seen in pachyonychiacongenital, must be soaked in warm water before they can be cut, to prevent irregular chipping. Nail conditioners should be applied for 2-3 months
Brittle nails:
Brittle nail results due to dehydration if nail plate water content is less than the normal 18%. They can manifest in the formonychorrhexisoronychoschizia. a. Onychorrhexisis excess longitudinal ridging. It has diverse etiologylike iron deficiency anemia and peripheral vascular disease which is due to hypoxia of the matrix; endocrinologiclike hyperthyroidism; metabolic disorders; psoriasis and may be idiopathic. b. Onychoschizia is splitting of the nail plate, usually along a plane that divides the thickness of the nail plate in to the superficial one third and deep two thirds, with frequent flaking. The cause of this disorder is most often chronic dehydration and rehydration of the nail plate, which may be experienced by people involved in dishwashing or gardening or by those whose profession requires frequent hand washing. It may also be due to poorly formed manicure.
Cosmetic Treatment:
- Wearing protective gloves with cotton lining can minimize contact with water and chemicals. Nail conditioning with alpha-hydroxy acid preparations or glycerine or application of nail enamel to both the top and underside of the nail plate decreases the surface area exposed to the atmosphere, thereby reducing water loss.
- Mechanical measures that act to reduce trauma to the nail include buffing and filing with an emery board to smooth the free edges, thus reducing the likelihood of inadvertent catching and tearing of the nail plate. Trimming and filing should take place after the nails have been well hydrated or after they are polished and let dry.
Hang nails:
Hang nails are common in nail biters but may also result from injury. Hang nails consist of small portions of horny epidermis breaking away from the lateral nail folds. The splits become painful when they penetrate to the underlying dermis.
Cosmetic treatment:
Frequent use of cuticle creams can prevent hang nails

Hang nail
Habit tic deformity:
It is a nail dystrophy which occurs as a result of self-induced habit when one rubs the central portion of the proximal nail fold of the thumb with the ipsilateral index fingernail consciously or inadvertently. It manifests as central transverse depressed lines of the thumb nail plate.

Habit tic deformity with central Beau`s lines.
Cosmetic treatment:
Spontaneous resolution occurs if the patient stops injuring the nail matrix.Nail sculpture and conditioners are the good cosmetic options till the nail grows normally.
Oral supplements for nail strengthening
There is no evidence based- data proving that oral supplements are effective. However, vitamin supplements, oligoelements, and aminoacids could be sometimes useful in certain nail disorders.
Vitamin E- 600-1200 IU daily for 6-18 months may induce a complete clearing of nail changes in yellow nail syndrome. Although the mechanism of action is still unknown, antioxidant properties of α- tocopherol may account for its efficacy.
Biotin (Vitamin H)- Can be useful in improving nail strength because it may help in the lipid molecule synthesis which produce binding between nail plate keratinocytes. Studies showing clinical improvement in patients who received biotin supplements have been documented.
Iron- It can be very effective in improving nail fragility.It is recommended when ferritin levels are below 10ng/ml.
Cystine- May be useful in promoting proper finger nail growth, hardness, and functionality.
Role of government and nail salons to ensure safe nail aesthetic service:
- It is necessary to establish national guidelines to nail art salons.
- Nail technicians should be licensed to perform services only on healthy nails and skin.
- Qualified dermatologists opinion should be soughtif a person has visible abnormal skin or nail conditions.
- Nail art technicians should be well trained on universal precautions to avoid blood borne infections.
Nail cosmetics are useful to disguise and conceal nail imperfections and unsightly dystrophies. Although many of the cosmetic products offerpalliative therapy of nail disorders, they may also be a source of significant adverse effects. There is a general lack of proper information and/or advanced training on use of nail cosmetics.Education of manicuristsand the public about the safe salon methods is vital in preventing complications.
Quick Links
 |
||
 |
||
 |
| Feedback | Admin Login |
| © 2020 Dr. Umashankar's Dermavision®. All rights reserved |
| Powered by Beyondrays |